Options for Enhancing New York's Health Home Initiative
A Discussion Paper
New York State’s Medicaid program, which serves more than 6 million residents and costs more than $72 billion annually, has been undergoing a complex and challenging, yet largely successful, redesign over the past seven years under the leadership of a stakeholder driven Medicaid Redesign Team. The goal has been to promote the “triple aim” of improving access, enhancing quality, and reducing cost. Key strategies have been expanding managed care services to a growing population and the development of delivery system reforms. A 2016 report by the Citizens Budget Commission (CBC) found these efforts had increased enrollment, lowered per enrollee costs, and promoted better outcomes for those served.1
However, some elements of the redesign plan have faced challenges in their implementation. Two efforts at delivery system reform, developing Performing Provider Systems (PPS) with links to community based organizations (CBOs) and using Health Homes (HH) to enhance coordination of services for those with complex care needs, have proved more challenging than initially expected. With support from the New York Community Trust, CBC has been exploring options for identifying improvements to these initiatives. A discussion forum among major stakeholders based on an options paper prepared by CBC staff on ways to promote greater CBO engagement in PPSs was held in November 2017.2
This paper addresses the challenges in extending HHs to all who can benefit from their services in a cost-effective manner. New York has more than six years of experience with its HH initiative and much has been accomplished. Since the launch in 2012 multiple new HH entities have been established, and current enrollment exceeds 175,000 people. A compelling combination of common sense and abundant individual examples indicates the care coordination and social service supports provided by HHs lead to better outcomes and long-run cost savings for many with complex conditions. The policy question is not whether HHs “work.” HH’s do work and should be sustained; they are making a contribution toward promoting the triple aim.
The more difficult and complex policy issues are for which types of eligible patients are HHs most cost effective and how those patients can be identified and engaged. Much remains to be done if HHs are to deliver the full potential of their benefits. With respect to numerical goals the current enrollment falls short of an initial three-year target of 240,000 and a larger long-term goal. Perhaps more importantly, little has been learned about whether such targets are appropriate based on evidence about the differential cost-effectiveness of the program for diverse subgroups. Those currently enrolled likely differ in important respects from those initially assigned priority for enrollment, and the cost-effectiveness of the program for the full range of patients being enrolled has not been demonstrated (although those served typically do benefit from an altered mix of services).
This paper explores options for setting priorities among the groups to be served by the HH program and more effectively reaching and enrolling those who can receive the greatest benefits. While a fundamental concern is the need for more complete and carefully analyzed data about cost savings among those served, the paper presents options for discussion based on the evidence available and the experience with enrollment to date. It should be noted that the analysis is relevant primarily to adults in HHs, because the State did not receive federal authorization for a separate children’s initiative until December 2016.
The paper is organized in five sections. It begins with a description of the HH intervention and how its approach to coordination of care for those with complex needs differs from earlier and parallel initiatives to improve care management. The next two sections present the initial plan for HHs in New York and how it has been modified in response to experience. The fourth section extracts relevant lessons for New York based on analyses of HH programs in other states. The final section presents options for future program modifications in New York while more extensive analysis of cost-effectiveness is undertaken. The suggested options are:
- Better targeting of priority subpopulations;
- Greater reliance on specialized HH entities;
- Stronger ties between HHs and Managed Care Organizations (MCOs);
- Alternative payment rates for HHs;
- Centralized development of marketing and training materials; and
- New initiatives to encourage interoperability of HH, MCO, and provider electronic health records.
BACKGROUND: THE HEALTH HOME AND OTHER MODELS FOR CARE COORDINATION
It has long been recognized that individuals with complex physical and behavioral health care needs may require, and likely would benefit from, assistance from specially trained staff in accessing and coordinating the services they receive from multiple medical care providers and in gaining access to social services that enable them to function in the community more effectively.3 Less clear are the best models for providing this service to groups with varying degrees and types of needs.
The current HH model for coordinating care was established in the federal Affordable Care Act (ACA) of 2010. It authorized State run programs to serve Medicaid enrollees meeting one of these criteria: adults having a severe mental illness (SMI) or children having severe emotional disturbance (SED), having HIV/AIDS, having two or more chronic conditions, or having one chronic condition and at risk for another.
The HH is required to provide eligible individuals with six services: (1) comprehensive care management, which typically includes preparation of an individual care plan integrating physical and behavioral health services; (2) care coordination, which typically involves assistance in implementing the care plan with services such as tracking referrals, aid in keeping appointments, and medication monitoring; (3) health promotion, which typically includes patient education and development of self-management plans; (4) comprehensive transitional care, which typically relies on hospital liaisons to notify the HH of hospital admissions and discharges and includes post-discharge home visits and medication compliance updates; (5) individual and family support, which typically includes referrals to peer support groups and advocacy with social service agencies on behalf of clients; and (6) referral to community and social supports, which includes referrals to community based resources and referral followups as well as assistance with housing. These services should be linked, as appropriate and feasible, by health information technology.4
The federal requirements with respect to the organizational form of the HH are flexible. The HH may be based in the office of a primary care physician, a behavioral health provider, or in other settings that suit the beneficiaries’ needs. The HH is typically a separate legal entity from medical care providers and receives a separate per member per month (PMPM) fee for the package of HH services. Federal staffing requirements are also flexible with no requirement for maximum caseloads and minimal educational or training requirements for care managers and care coordination staff. States may create separate HHs for different categories of beneficiaries such as those with SMI versus others or children versus adults.
The ACA provided a financial incentive for states to create HHs. It authorized federal cost sharing for HH payments of 90 percent for the first two years of enrollment of the eligible population. The usual federal Medicaid share varies among states and is 50 percent for New York.
Prior to the ACA New York State agencies had established models for care management for distinct populations. For nearly a decade four programs evolved to enroll about 35,000 Medicaid beneficiaries before the HH initiative was launched, and these programs had standards and practices similar to the HH model.5 Three of the programs served distinct specialized populations. A Targeted Case Management (TCM) program sponsored by the Office of Mental Health included about 150 organizations statewide which provided care management and coordination to selected adults with SMI and children with severe emotional disturbance. Referrals to the program were made by the local (county or New York City) public agency responsible for mental health services. TCM providers received monthly per recipient fees under Medicaid.
The Office of Alcoholism and Substance Abuse Services supported a Managed Addiction Treatment Services (MATS) program for high-cost, high-need individuals with substance use disorders. The Office funded “slots” at eight agencies, three of which were in New York City and one each in five other counties. The local government was responsible for referring patients to the providers.
A third program served HIV-infected persons also diagnosed with a mental illness, substance use disorder, or at an advanced stage of illness. It had 46 provider organizations statewide with 34 in New York City. The agencies could bill Medicaid for their services.
Unlike the other three programs, the fourth initiative, the Chronic Illness Demonstration Project (CIDP), was not intended as an ongoing activity but was established as a temporary demonstration.6 It operated for three years spanning 2009 to 2012. The target population was Medicaid enrollees not in an MCO and with a high probability of being hospitalized in the coming year largely due to multiple chronic conditions. Six organizations were approved to provide services, three in New York City and one each in Nassau, Westchester, and Erie counties. The three New York City agencies were authorized to enroll up to 500 people each; the other agencies were approved for 250 each. The organizations were paid monthly fees for each individual enrolled, and they were responsible for recruiting eligible patients.
An evaluation of the CIDP completed after the three-year demonstration found important objectives were not met. The enrollees had utilization rates for hospitalizations and emergency department visits similar to a control group, and their overall Medicaid costs were somewhat higher due to the added costs of coordination. In discussing the findings the evaluators noted the costs could become lower in subsequent years and that quality of care and patient satisfaction were not measured in the study and may have improved. They also observed that the participating agencies did not uniformly follow best practices including frequent in person contacts, access to timely information about emergency department use, and close interaction with primary care providers. Another important finding was that the agencies devoted substantial resources to recruitment efforts and still fell short of their authorized enrollment targets. In addition, Department of Health (DOH) regulations and practices added to enrollment difficulties. Lessons drawn from that finding indicated that any future efforts should provide considerable resources for outreach and better procedures should be developed.
When the New York HH initiative under the ACA was designed, the plan was to have each of the predecessor programs become part of the new HH program. The State would benefit from the 90 percent federal reimbursement for payments to the programs. The current patients could continue, and over a two-year period the agencies would be converted to the new HH rate structure but assured at least their previous rates during the transition. New referrals to the programs would follow the new HH process.
At the same time the State was planning to merge specialized case management programs into the HH initiative, it also was continuing Medicaid support for the Patient Centered Medical Home (PCMH).7 In 2010 New York’s Medicaid program began making supplemental payments for services by a provider who had qualified as a PCMH.
The PCMH is a national model defined by standards first set by the National Committee for Quality Assurance (NCQA) in 2008 and subsequently revised in 2011. It is intended to serve patients with less intensive needs than those targeted by health homes. The NCQA designates a primary care medical practice (which can be a private physician group practice, a community health center, a hospital clinic, or other organization) as a PCMH when it meets multiple standards including broadened access through extended hours of operation, a team approach to care delivery, coordination of care transitions and referrals, and personalized care management for complex, chronically ill patients. Although a PCMH may serve many patients who are not chronically ill or otherwise eligible for a Medicaid HH, many HH eligible individuals may be enrolled in a PCMH. For those people the HH provides additional services, but some of the core HH activities overlap with PCMH standards.
The supplemental Medicaid payments helped stimulate substantial growth in the PCMH program in New York. By July 2013 more than 4,900 providers were PCMHs, and in April 2016 the number reached 6,264 and an estimated one-quarter of all primary care physicians statewide were practicing in PCMHs. Of the total PCMHs about 45 percent were in New York City. Statewide about 55 percent of the PCMHs were based in health centers or hospital clinics (where Medicaid patients concentrate) and large private group practices were about one-quarter (other forms include small groups and other practices); in New York City hospital clinics (including those of the municipal hospitals) and health centers were nearly three-quarters of the PCMHs. The growth in hospital based PCMHs was stimulated by a $250 million federal grant program during 2011 to 2014 to support transformation of hospital clinics in New York to PCMHs as well as the State supplemental Medicaid payments.
While PCMH and HH are the two major care coordination models supported by New York’s Medicaid program, the federal Medicare program has also been encouraging development of better care management with additional models. This impacts the Medicaid program because about 700,000 New York Medicaid enrollees are “dual eligibles” enrolled in both Medicaid and Medicare, and this group includes many seriously ill individuals who may qualify for HH services or be served by a PCMH. Dually eligible enrollees deserve considerable attention in efforts to improve care and reduce costs; although only 15 percent of the State’s Medicaid enrollees, they represent 27 percent of the program’s cost.8
The most notable Medicare initiative is the Accountable Care Organization (ACO) program. ACOs are networks of providers who agree to deliver services to a defined population of Medicare enrollees. They are paid under the Medicare fee-for-service arrangements, but annually can receive additional payments based on savings achieved relative to the cost of comparable enrollees not in the ACO. Savings are expected to be achieved through greater care coordination resulting in reduced hospital admissions and reduced emergency department use; in addition, quality of care is expected to improve through greater service coordination, patient involvement and patient education, and outreach. Multiple versions of the program have been offered with the ACO’s potential bonus varying depending on the degree of risk it accepts for potential losses due to higher costs than the comparison group. Nationally the number of ACOs increased from 220 in 2013 to 561 in January 2018 with 10.5 million Medicare beneficiaries in the program at the start of 2018.9
In New York State the number of ACOs has grown from 1 at the start of the program in 2012 to 16 in 2013, 22 in early 2014, 32 in 2016, and 36 in 2017.10 Combined enrollment in 2016 was more than 576,000 with individual ACO enrollment varying from under 6,100 to more than 74,000. In New York approximately one in five Medicare fee-for-service beneficiaries is enrolled in an ACO. The ACOs in New York have had difficulty achieving savings. In 2016 only five of the 32 ACOs received bonus payments; the rest had savings too small to qualify or had losses (that is, their expenses exceeded the benchmark). As a group the ACOs generated a net loss of $60 million or about 1 percent of benchmark spending. The 2015 results were similar; 29 ACOs generated a net loss of $64 million.
Medicare also experimented with greater care coordination through the Comprehensive Primary Care Initiative (CPCI), a four-year nationwide demonstration begun in 2012. The demonstration involved 502 primary care practices in seven regions of the United States (including the Hudson Valley-Capital District in New York). The practices agreed to make changes to promote case management and patient engagement with the goals of improving quality and reducing costs; the practices were not required to be PCMHs, but the two initiatives did overlap. As a financial incentive for the changes, the practices received case management fees during the first two years that varied from $8 to $40 per month per beneficiary based on the patient’s acuity. An evaluation of the first two-year experiences found that practices were initiating changes in their processes but found no statistically significant changes in most quality of care measures and negative changes in spending (that is, spending was higher) for the participating Medicare beneficiaries compared to matched Medicare fee-for-service patients.11 Since the evaluation spanned only a relatively short term, the findings with respect to cost and outcomes should be interpreted cautiously.
Another demonstration involving Medicare enrollees was conducted at the HH at Maimonides Medical Center in New York. It received a $14.8 million grant spanning a three-year period (2012- 2015) to serve 7,500 people with SMI including 500 Medicare beneficiaries by coordinating their physical and behavioral care. An independent evaluation found the program was implemented successfully with almost all participants receiving care management services, and the “care managers built strong and consistent relationships with participants and played key roles in helping them find and maintain housing and connect with other social supports.”12 With respect to savings, among the relatively small number of Medicare beneficiaries, no statistically significant differences were found between the Medicare enrollees and a comparison group of fee-for-service Medicare beneficiaries with similar conditions for total costs, hospital admissions, and emergency department use. With respect to the Medicaid enrollees, the comparison group was other Medicaid enrollees with similar conditions in other HHs; the findings were that both groups had increases in spending after enrollment, but the increase at the Maimonides HH was lower. Thus, relative to other HHs, the demonstration project was credited with savings averaging $944 per beneficiary per month.13
A final observation about the Medicare ACO initiative is that it focuses on beneficiaries who rely on fee-for-service payments. Medicare beneficiaries in the Medicare Advantage program, which relies on managed care plans receiving capitation premiums for Part A and Part B services, are not eligible for the ACO program. The assumption is these managed care plans already have a financial incentive to coordinate care effectively, and additional incentives are not necessary. In New York State more than one-third of Medicare beneficiaries are enrolled in Medicare Advantage plans.14 This approach contrasts with the strategy for Medicaid HHs. Medicaid enrollees in both fee-for- service arrangements and in Medicaid managed care plans can enroll in a HH because the managed care plans (which serve about 77 percent of all Medicaid enrollees in New York) have limited resources for care coordination and most often confine their efforts to telephone contacts and do not engage in the face-to-face contacts intended to be an important element of HH activities.
NEW YORK’S INITIAL HEALTH HOME DESIGN
New York was one of the earliest states to establish a Medicaid HH program under the ACA. The program was authorized in the State budget adopted in March 2011. DOH staff designed a program in subsequent months and submitted a proposal to the Centers for Medicare and Medicaid Services (CMS) in November 2011. The plan was to be launched in January 2012 in 10 counties (including Bronx, Brooklyn, and Nassau), expanded to another 13 counties (including Manhattan, Queens, Staten Island, Suffolk, and Westchester) in April 2012, and to the rest of the state in July 2012. CMS approved the plan on February 3, 2012 retroactive to January 1, 2012. The initial State Plan envisioned the HH program would be expanded over time to serve children and the developmentally disabled.
Individual Eligibility
The plan took a broad approach to eligibility. Based on applying the federal criteria to the 2010 Medicaid population of about 5 million, at least 975,000 enrollees were estimated to be eligible. Within this group the largest number, about 409,000, experienced mental health issues or substance use disorder; 111,000 qualified solely on the basis of severe mental illness, and the others had less severe mental conditions and accompanying chronic conditions. Among the total group with multiple conditions, 52,000 had developmental disabilities, 55,000 had HIV/AIDS, and nearly 210,000 were receiving long-term care services. Among the total eligible population nearly one-third (32 percent) were dually eligible for Medicare and Medicaid, and just more than half (51 percent) were enrolled in a Medicaid managed care plan.15
The State’s plan did not call for enrolling all 975,000 people estimated to be eligible. (See Table 1.) Individuals with developmental disabilities and those receiving long-term care services were deferred pending development of specialized arrangements for them.16 Priority was assigned within the remaining group based on need for care coordination as measured by a Clinical Risk Group score based on the acuity of their conditions, prior service utilization, and adjustment for factors such as severe mental illness and HIV/AIDS status. Based on these scores the target population was refined to include 509,000 individuals who would be given priority in the first three years. This group was further divided into three groups based on the cost of their care (high, middle, and low); about 270,000 were in the low-cost group and highest priority was given to the other 238,000 with the higher costs. At least these 238,000 were targeted for enrollment by the end of September 2015.17

This initial approach to setting priorities had a clear and justifiable logic, but in retrospect, operationalizing the list as intended revealed practical flaws. The underlying data was not always as accurate or as up-to-date as desired, the acuity index may not have been the most appropriate one, and focusing on a high-cost and high-acuity population would raise outreach and enrollment challenges for the new HHs.
HH Qualifications and Performance Standards
With respect to criteria for entities to qualify as HHs, the State emphasized fostering a newly created network of relatively large and comprehensive entities. The previously established care management programs described above were grandfathered into the program as “legacy” agencies, and they were expected to expand beyond their current relatively small population with new enrollees and broaden the scope of their activities. The legacy agencies were seen as essential for continuity of care for their patients and for their experience in serving high needs populations, notably those with SMI and HIV. They were also seen as having shortcomings relating to and coordinating with physical health providers that needed to be rectified.
Primary emphasis was given to newly created lead HH organizations to enroll large numbers of those eligible and be accountable for HH service delivery. The organizations would have to meet the federal criteria of providing the six core services and making use of appropriate information technology. The State required lead HHs to develop a comprehensive network of agencies that could serve a broad population with a variety of conditions including mental illness and a range of chronic conditions; specialized HHs serving a narrow population were not encouraged. The State received 165 letters of intent from entities seeking to become HHs; collaboration was encouraged and at the start of the program 32 organizations were designated as lead agencies.
The HHs were new entities, but typically consisted of previously existing providers brought together in a new form of collaboration. The responsibilities of the HH lead agency were to provide overall management and administrative services; to contract with care management agencies (some of which were operated by the lead agency) which performed outreach and care management; and build a network of affiliated providers including physician services and social service agencies. Most of the lead agencies are long established Medicaid providers.
In New York City, Long Island, and Westchester County 15 HHs operate with recent enrollment totaling more than 100,000. (See Table 2.) Ten of the HHs are affiliated with a hospital system, including two HHs – Queens Coordinated Care Partners and Mount Sinai Health Home Serving Children – affiliated with the Mount Sinai Hospital system. The five others are not affiliated with hospitals. The unaffiliated health homes were born from a variety of avenues, including CBOs and collaborations among pre-existing care coordination providers.

The State required HHs use a multidisciplinary team approach and that the team be headed by a person dedicated to case management. No required standard was set for maximum caseload– intending to provide care managers flexibility to meet the varying needs of a mixed caseloads, but information relating to rate-setting indicated an assumed ratio of adult enrollees to the case manager of 91:1 statewide, ranging from 12:1 for those with the most severe mental illness to 116:1 for those with two chronic conditions and low acuity.18 Subsequent rate revisions described below support caseloads ranging from 20:1 for those with high acuity and mental illness to 77:1 for those with low acuity and without mental illness conditions.19 The State established minimum educational requirements for case management staff and for those administering assessments.
Once in operation the HHs would have to report regularly to DOH on their activities. The tracked data include the numbers of people in outreach status and enrolled and the numbers receiving each of the five required services each month. In addition the DOH plan anticipated using administrative data on service claims to track for enrollees several quality and outcome measures including rates of inpatient acute care use, rates of emergency department use, rates of followup visits for certain hospital discharges, medication management and adherence for those with mental illness, asthma, diabetes and certain other conditions, and receipt of the preventive services of colorectal cancer screening and chlamydia screening for women.20 The plan also anticipated eventual estimates of costs savings from HHs using claims data and econometric techniques applied to a comparison group.
Enrollment Process
The enrollment process for the HHs was voluntary on the part of the Medicaid patients. The HH’s affiliated care management agency would reach out to eligible individuals, and they would have to take affirmative action to agree to receive HH services and sign a consent form. This contrasts with alternative models of mandatory enrollment (under which clients are obliged to choose a HH or be assigned to one) and passive enrollment (under which clients are initially assigned to a HH but can choose to disenroll or “opt out”). Voluntary enrollment was viewed as most appropriate because it promoted empowered choice, and the program was not likely to be effective with clients who did not want to be cooperative.
The bulk of new enrollment during the initial years was expected to take place through a “top down” process. DOH would identify the priority eligible enrollees based on the previously described cost and acuity criteria including predictive risk scores related to future negative outcomes such as hospitalization, nursing home admission, and death. Their identity and other information would be provided to the most appropriate HH. If the Medicaid beneficiary was enrolled in an MCO, then the MCO would recommend a specific HH, and the HH would be informed through the DOH centralized tracking system. If the priority enrollee was not in an MCO, then DOH would send the information to a HH it selected based on the individual’s prior use of service and conditions. In either case the HH’s care management agency was expected to reach out to the individual, inform them of the benefits of a HH, and obtain their consent on a voluntary basis to enroll in the HH.
The plan also permitted “bottom up” enrollment. A HH’s affiliated care management agency and medical providers could identify individuals they believed would benefit from the HH services. This typically would take place in community based clinics or hospital emergency rooms, where the HH network agencies have staff located. In this process the care management agency staff would provide the HH lead agency (and MCO, if relevant) with information about the patient, and the lead agency would use the information to verify eligibility and appropriateness for HH and refer the individual to DOH to approve (or disapprove) enrollment in the HH.
Enrollment practices for children differed from those for adults. No top down referrals were made for children because of complications related to the need for parent or guardian approval. Local social services districts and foster care agencies could refer potentially eligible children to a HH. The HH then gathers documentation to prove eligibility and submits the enrollment to the State.
The plan also indicated that hospitals should make a referral for HH enrollment for patients admitted through the emergency department. The referral would be to the MCO in which the patient was enrolled (which would then recommend a HH for referral) or directly to a HH with which they were associated if the patient was not in an MCO. The HH’s affiliated care management agency would then be responsible for reaching out to the patient and obtaining their voluntary enrollment.
Payment Rates
The DOH established two types of payments for HH services. The basic ongoing revenue stream would be PMPM payments for enrolled individuals. The payments would vary with location (downstate versus upstate region with downstate rates somewhat higher) and the individual’s Clinical Risk Group score.21 Higher acuity patients would carry higher payments, and each patient would have a specific rate tied to his or her acuity. The range of monthly payments based on acuity varied from $32 for an upstate patient with diabetes and hypertension to $413 for a downstate patient with high severity HIV disease.22 This payment rate structure was designed by DOH in consultation with key stakeholders.
For patients in an MCO the payment from the State would flow through the MCO, and the MCO was entitled to retain up to 3 percent of the money for its administrative costs.23 For enrollees not in an MCO, the State payment goes directly to the HH lead agency (or to the pre-existing legacy provider in the case of the grandfathered agencies). The bulk of the payments received by the HH lead agencies is paid to the affiliated care management agencies with the amount a HH lead agency can retain for administrative and other services limited by DOH regulations.
In keeping with the lesson learned from predecessor care coordination initiatives, DOH established meaningful outreach rates in addition to PMPM rates. For the top down referrals, the HH would receive monthly payments to find and sign up the patient. The rate was set at $135 monthly. A HH could receive the outreach rate for up to three months, after which the individual would either be enrolled or the HH could no longer collect the outreach payment. However, after a three month wait, the HH could again initiate an outreach effort for which it would be paid up to another three months.
One additional refinement is that separate rates were set for the legacy agencies providing case management services. These agencies received rates equivalent to their previous per patient revenue for a two-year transition period as they qualified as HHs. After that period they would receive payments on the same basis as other HHs, which were lower than their legacy rates.
IMPLEMENTATION EXPERIENCE AND PLAN MODIFICATIONS
Implementation of a complex public program almost inevitably requires modifications along the way, and such changes can be constructive responses to unanticipated circumstances. New York’s HH initiative has been refined in four significant ways: (1) changes have been made in the payment rates and payment process to create more appropriate incentives and to reduce payment delays and inequities; (2) enrollment difficulties have been addressed by modifying targets and relying more heavily on bottom up enrollments; (3) a need for new specialized HHs for children was recognized; and (4) use of performance measures to promote HH accountability was delayed with a relatively sophisticated (but still imperfect) set of metrics put in place in early 2018.
Adjustments to Payment Rates and Processes
During program implementation the payment scheme initially designed showed some flaws and corrective actions were taken. This includes multiple adjustments to the payment amounts and changes in the payment process with significant MCO, HH, and care management agency stakeholder involvement.
Rate Changes. The basic principle that rates would reflect location (upstate and downstate) and the patients’ acuity has remained in effect, but adjustments have been made to make the structure more effective. Initially acuity scores were assigned to each patient, and the average acuity score of a HH’s enrollees set the monthly payment to the HH. This was modified in October 2012 so that HHs (excluding legacy providers) billed separately for each enrollee, and each enrollee had a specific rate based on their acuity score.24
Beginning in April 2014 rates were temporarily increased for three years due to the availability of designated funds as part of the federal-state waiver known as the Delivery System Reform Incentive Payment (DSRIP) program. It provided up to $8 billion in federal funds of which $6.4 billion was for the development of 25 PPSs statewide to execute multiple projects to reduce unnecessary hospital use; the other funds were for a variety of activities and included $190.6 million in federal and state funds for HH Development Funds. These funds were distributed as an add-on to the rates based on the HHs committing the money to development of necessary infrastructure including information systems.25 Also noteworthy is that among the projects undertaken by some PPSs were efforts to expand HH services to people not meeting the federal eligibility criteria but at risk of qualifying and seen as likely to benefit from better care management.
Effective July 1, 2015 the rate structure was revamped to a simplified structure. The changes were made based on stakeholder recommendations for simplicity. Instead of each enrollee having a specific rate based on their acuity score, the enrollees were assigned to one of three levels (high, medium, or low) of acuity and common rates established for each of those levels. The assignment to a level remains based on an individual’s acuity score, but only three basic rates were applied. Differential rates were also established for clients with significant behavioral health problems who are enrolled in an MCO’s enhanced Health and Recovery Plan (HARP) to integrate mental and physical health services.26 Refinements to rates were set also for relatively small groups who were in adult homes or transitioning from inpatient psychiatric care or prisons (dubbed Health Home Plus).27 The previous outreach rates remained in effect.
Although the previous targeted case management plans had been “grandfathered” into the HH program and guaranteed their previous rates for a two-year transition period, this transition was extended. In February 2013 DOH extended the rates until two years after the provider had converted to a health home, creating varying ending dates.28 Through multiple subsequent extensions, legacy rates were aligned and extended through November 30, 2016.29 Beginning in December 2016, all HHs including the former legacy agencies were brought under a uniform rate structure. As with other rate changes, the extensions and transition involved notable stakeholder involvement.
Effective May 1, 2017 the rates for the low acuity enrollees were increased.The table below summarizes these adjustments.

This increase responded to pressure from HHs who argued the low acuity rate did not support adequate staffing and services. In addition the low acuity rate was less than the outreach rate, creating a financial incentive for HHs to extend low acuity patients’ outreach status rather than enroll them promptly.
Effective October 1, 2017, the monthly outreach rate was decreased from $135 to $110. This reduction was a response to legislative pressures during the annual budget process for program savings, and a DOH belief that the rate was generous relative to the activity required and a concern about lower return on investment from outreach as time went on since program launch. The rate change was accompanied by changes in the protocols for outreach. Rather than three months on, three months off, three months on construct for outreach payments, the timeframe was reduced to two months with a face-to-face meeting required in the second month of outreach for it to be billable.30
Table 4 below summarizes the current rate structure.

Payment process changes. The payment process for people enrolled in MCOs, about 73 percent of HH enrollees, did not work smoothly.31
The payments were intended to flow from DOH to the MCO and then to the HH and its contracted care management agency or agencies. Billing and payment were often delayed due to multiple potential glitches in the flow of required information including gaps in information supporting eligibility from the HH lead agency and its care management agency, inadequate billing procedures by the MCO, and inaccuracies in the database used by the DOH to verify information. As HHs and affiliated care management agencies encountered cash flow problems they voiced complaints, and effective December 2016 DOH changed the arrangement so that billing and payments took place directly between the HHs and DOH, eliminating the “middleman” step of MCO processing.32 (Not coincidentally, this was also the date when legacy providers were shifted to the standard HH rates,
allowing them to continue billing independently for their funds.) The adjustment was intended to be brief and temporary as a streamlined process was designed to make the flow through the MCOs quicker and easier. Effective in May 2018 payments for HH services will be included in MCO capitation rates, and the MCOs will make the payments to the HHs. The MCOs are required to pay state established HH rates, but some flexibility is allowed if an alternative relationship is agreed to as part of a value based payment arrangement between the MCO and the HH.
Annual spending on HHs grew from $87 million in 2012 to $558 million in 2017, due primarily to enrollment growth discussed below. (See Table 5.) Spending on those enrolled (including legacy providers) rose from $84 million to $396 million over this period. Of the $396 million spent on enrollees, 60 percent was for non-HARP adults, 23 percent for HARP adults, 12 percent for children, and 5 percent for others.
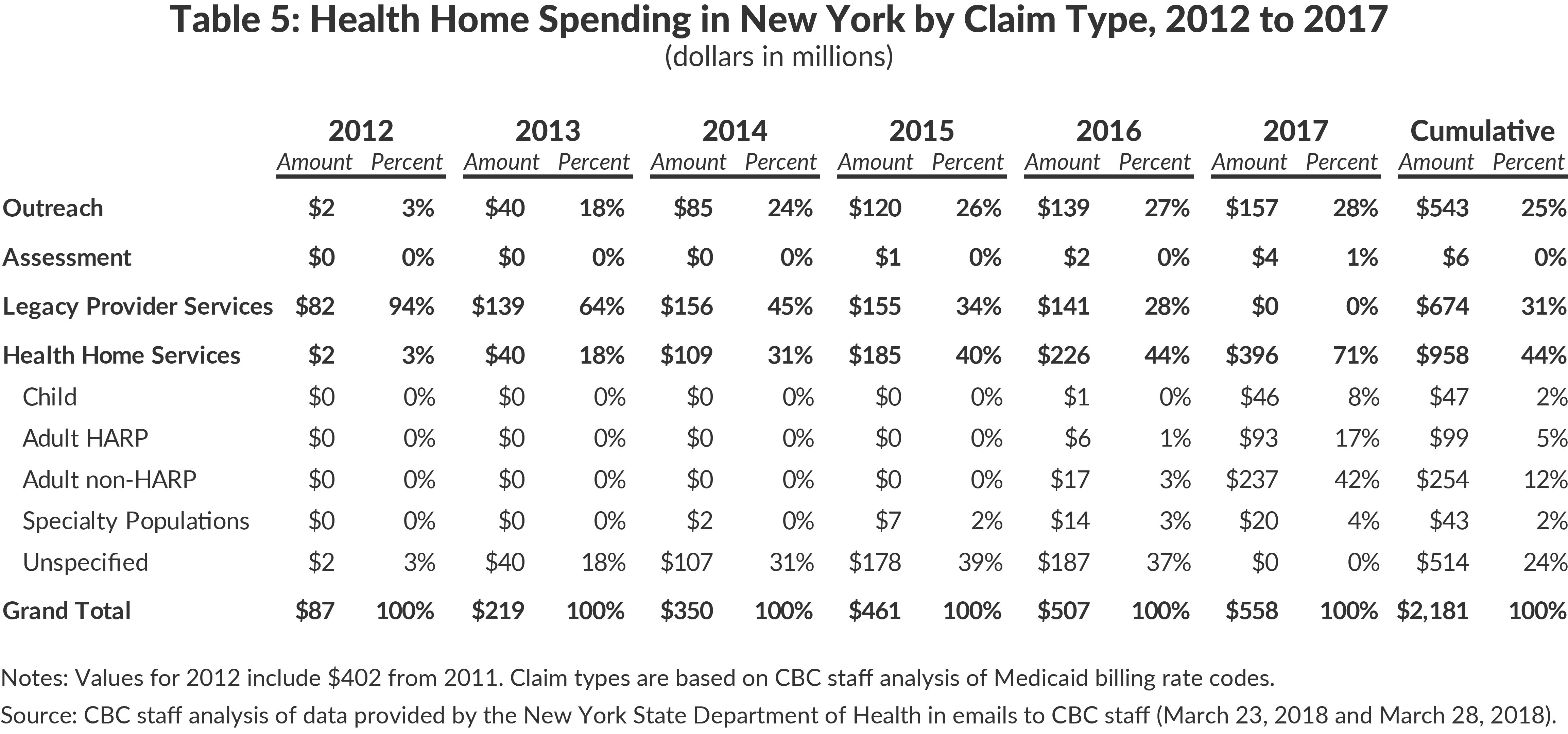
Outreach payments represent a substantial portion of total spending, amounting to $157 million, or 28 percent of the total, in 2017. This share of spending on outreach is consistent with the previous three years, but is expected to be lower going forward due to the reduction of the outreach rates and new procedures effective October 1, 2017. The cumulative $543 million spent on outreach represents a large scale effort that has sought to engage a large number of complex need, high acuity consumers of health care services with limited success.
Problems with Enrollment
As described earlier, the initial plan assigned priority for enrollment in the first three years to 238,000 relatively high-cost and high-acuity Medicaid clients, with another 270,000 lower cost beneficiaries to be assigned after the first tier patients were enrolled. As shown in Figure 1, actual enrollment has lagged those targets. After three years enrollment reached about 116,000 or less than half the target for the highest priority group. Subsequently enrollment has risen to about 176,000, still well below the initial target after more than six years. In order to promote the benefits of HHs it is important to understand the reasons for lower than anticipated enrollment and design measures to bring the program to all who might benefit cost effectively.

A major factor in the low enrollment was the ineffectiveness of the top down enrollment process. While the state sought to arm HHs with data on member predictive risk and clinical acuity to better target care management to the most needy, practical issues emerged with the available data. The care management agency outreach workers relied on information supplied by DOH. This information, coming from the old eligibility and enrollment system (prior to the building of better data through the more modern health exchange) was often outdated or inaccurate with respect to the current address and phone contact of Medicaid clients, making it difficult to locate them. Once an outreach worker found a potential client, it was difficult to obtain voluntary enrollment, because clients were often confused about the nature and benefits of a HH. The term “health home” often made clients believe they would have to go to a specific place and led to confusion between HHs and home care services. Others who better understood the nature of the service (or where the service was not fully explained by an MCO currently providing telephonic care coordination) may have felt they were already served by their MCO or primary care provider. The issues related to locating and informing clients were particularly difficult for those with SMI (many of whom are unstably housed), who comprised a significant proportion of the top down referrals.
Another anticipated source of enrollees was referral from hospitals, whose staff were expected to refer Medicaid clients meeting HH eligibility criteria and using emergency rooms or admitted to inpatient services. However, this provision was not rigorously adhered to by most institutions, and the timeliness of referrals made was often problematic. HH outreach workers would not get information about a client in the emergency department or discharged until well after the fact, and locating them outside the hospital could be challenging. In February 2017 DOH issued guidance to hospitals specifying expected procedures for making referrals to HHs and indicating that enforcement measures would be taken.33 Since then the volume of referrals has increased, often with assistance from organizations participating in PPSs.
Given these challenges, a significant proportion of enrollment was through the bottom up process. HH lead agencies and care management agencies stationed workers at hospitals to recruit members at the emergency room or clinics, at community health centers, and at field locations such as homeless shelters frequented by likely eligible individuals. In addition providers affiliated with HHs such as community health centers and mental health clinics used their current patient rolls as a source of appropriate referrals. Contacts were more likely to be effective when made at service locations used by the clients and at times when clients were in need of services and could appreciate the benefits of HH activities, as opposed to cold calls generated by top down referrals. In some cases, such bottom up enrollment may actually be clients initially identified in the top down process who rejected enrollment at first contact.
The evolving enrollment process has resulted in an enrollment profile dominated by those with lower acuity. (See Table 6.) About 56 percent of all enrollees have lower acuity (still with multiple chronic conditions), with the shares ranging from 43 percent for adults in HARPs to 59 percent for other adults. Given the rate structure, a smaller share (25 percent) of the expenditures are for those with low acuity.

Creation of Specialized HHs for Children
The initial HH program design anticipated a phased-in approach to enrolling children. The cautious approach was based on a concern for the special needs of children and legal issues related to consent. HHs would need ties to pediatricians and relevant medical specialists as well as the social service, child welfare, and educational agencies for which children are the primary clients. Most agencies that were likely sources of bottom up referrals of children were not familiar with HHs and were reluctant to make referrals to these entities.
Early in the initiative planning was undertaken with stakeholder involvement to design an effective approach to enrolling and serving children. After obtaining federal approval for a specialized HH and additional specialized rates, in 2016 DOH launched new special HHs serving children. This was seen as a positive step in order to stimulate enrollment for children in HHs, to assure that the referral networks of providers were sufficient to serve children and youth, to add complex trauma as a criterion for eligibility, and to gain a 90 percent federal match for the new eligibility group. Distinct standards were established, the referral process was revised, and an assessment tool designed for children was required.34 Three new specialized HHs for children were formed during 2016, and as of December 2017 they had enrolled 9,247 children. (See Table 7.) Additionally, HHs serving adults were able to apply to serve children; of the 31 HHs currently serving adults, 13 also serve a total of more than 3,000 children.

Delay in Use of Performance Measures
Performance measures are useful at two levels of analysis – for the program as a whole and for individual HHs. For the program, the federal requirement for evaluation calls for assessing the impact on hospital inpatient utilization and costs, emergency room utilization and costs, skilled nursing home admissions and costs, and primary care utilization. Data on these metrics has been reported in accord with federal requirements which called for submission of data relating to 2012 starting in 2016 and periodically thereafter. In addition the State’s plan called for a more rigorous evaluation using comparison group or groups, and DOH has engaged the National Center on Addiction and Substance Abuse to support the analysis of claims and other data to determine the impact on costs and quality indicators. This evaluation is ongoing and no findings have yet been made public.
Data at the specific HH level is intended to hold organizations accountable for their performance and identify HHs for which technical assistance might help improve performance. In April 2016 DOH began, with the cooperation of HHs, developing a set of suitable performance measures for this purpose. In May 2017 DOH shared with HHs a preliminary design of performance and quality measurement, with new data collection efforts from HHs beginning in July 2017 to supplement existing administrative data.35 In January 2018 the first performance reports were released to HHs with data covering 2013 to 2016. Going forward reports are to be released every six months, and annual performance improvement goals have been set for each HH.36
The performance measures include four utilization measures for which performance goals have not been set (emergency department utilization, hospital inpatient utilization, mental health utilization and skilled nursing home admissions), and 28 measures for which goals have been set. The data for each measure for each HH and the improvement target for each HH were shared with the individual HHs in January 2018, but have not been made public. As part of a briefing for legislative members in March 2018, data for four indicators were made public.
The available data suggest two findings. First, a large majority of HHs show improvement on the indicators during the 2014 to 2016 period covered. Second, the performance of individual HHs varies widely. Among the four indicators for which data were publicly released, two had variations in 2016 between the high and low performance measures of more than 400 percent, with two in a more reasonable range of 60 percent and 20 percent.
The wide range in performance and other factors have led HH leaders to question the appropriateness of the metrics being used.37 Important limitations of the measures are: a lack of accounting for duration of enrollment of clients, a factor associated with program effects; a lack of adjustment for acuity of enrollees, a factor affecting some indicators; and the exclusion of data for dually eligible enrollees for most measures due to its unavailability, even though dually eligible enrollees account for a varying and significant share of individual HH enrollment. In addition the indicators are not adjusted for social determinants of health that may underlie variability among agencies, and meaningful baseline or comparison group indicators are not available to assess the performance of HHs as a group.
EXPERIENCES IN OTHER STATES
In addition to New York, 20 other states and the District of Columbia have established 32 HH programs. More than 1 million Medicaid beneficiaries are enrolled in these programs.38
Evaluation of the Early Programs
The federal Department of Health and Human Services commissioned an independent, five-year evaluation of 13 programs in 11 states including New York that started operation before the end of 2012.39 The evaluators classified the programs into three groups based on the strategy they followed. One group, comprised of four programs in Oregon, Missouri, Iowa, and Idaho, relied on pre-existing patient-centered primary care homes (PCPCH) to serve as the HH and paid them additional monthly fees for the expanded services. Three of these (Iowa, Idaho, and Missouri’s primary care program) were relatively small (less than 15,000 enrollees) due to the limited scale of eligible providers and beneficiaries. The larger program (more than 60,000 enrollees) in Oregon was supported by the state only for the two-year period of enhanced federal matching; in 2013 it formally ended the program and expected the PCPCHs to continue to provide coordination services without the enhanced payments. Idaho discontinued its program in 2016.
A separate analysis of the Iowa program by faculty at the University of Iowa under contract with the Iowa State Department of Human Services was published in 2016.40 Iowa’s program paid extra fees for HH services to PCMHs, who were able to select and passively enroll PCMH members who they thought were suitable for the HH program. Change in cost and emergency department use for 13 months before and after enrollment for HH members were compared to changes in cost and emergency department room use of similar Medicaid enrollees over the same period. The analysis indicated a 15 percent savings in cost for the HH members with greater savings for those enrolled in the program for more than one year. The favorable results were interpreted to be due in part to the ability of the providers to select those who were enrolled and thereby prioritize those most likely to respond to the program.
A second group of five programs in four states focused on a relatively narrow category of eligible people and relied on providers specializing in those conditions and often previously treating the enrollees to serve as the HH. This included two programs in Rhode Island, specializing in children and adults, respectively, with SMI; programs in Missouri and Ohio also limited to those with SMI; and a program in Wisconsin for those with HIV/AIDS. These programs were relatively small, ranging from 150 enrollees in Wisconsin to about 19,000 in Missouri. Each of these programs has continued beyond the period of enhanced federal matching.
The third group consisting of programs in four states including New York followed a strategy of seeking to serve a broad range of eligible clients through networks of providers including a case management agency. The North Carolina program achieved the largest enrollment, more than 525,000. However, the North Carolina program did not seek to create new care coordination entities and relied entirely on a pre-existing network (Community Care of North Carolina, or CCNC) and deemed all its current clients as HH enrollees. The evaluators reported: “No significant changes have been made to CCNC’s underlying structures, processes, enrollee assignment, provider requirements or payment rates as a result of the state’s adoption of the health home program. The state implemented the program administratively, using the enhanced federal match funding to defray Medicaid costs with no health-home related change in practice or payments...”.41
Maine’s strategy combined reliance on pre-existing PCMHs to qualify as HHs and serve the bulk of the eligible population but added a set of 10 new entities called Community Care Teams (CCT) to provide supplemental services to the top 5 percent of high-risk, high-cost patients. These patients are referred to the CCT by the PCMH providers. The monthly fee to the CCT is more than 10 times that for PCMH providers ($12.00 versus $129.50 per month). Maine has more than 50,000 enrollees in its program.42
Alabama’s strategy relies on two types of pre-existing entities. Eligible beneficiaries are enrolled with a primary care physician who typically was previously serving them and continues to play a role in coordinating care; however, each primary care physician is required to contract with a Patient Care Network of Alabama (PCNA) for additional case management services. The PCNAs are regional entities created in 2011 to support primary care physicians. The primary care physicians and the PCNAs are each paid a monthly fee for each enrolled beneficiary. The program began serving 21 counties and was expanded statewide in 2015; its enrollment exceeds 220,000.43
The independent evaluation sought to determine the HH programs’ impacts on quality and cost of care. Although most states had planned to conduct an evaluation, their efforts were limited. At the end of the fourth year the evaluators noted: “Although the program has been in place for four years in some states, its impacts on enrollee health outcomes, utilization of services, and costs remain largely unknown due to lack of reliable quantitative data.”44 Three states (Oregon, Rhode Island, and North Carolina) conducted no internal evaluations. Efforts in the other states were preliminary or incomplete, and these analyses had three limitations: (1) It was not possible to distinguish the impact of the HH program from that of other initiatives underway during the implementation period. (2) Available data covered only the early period of implementation and often did not include a pre-implementation baseline. (3) The data available excluded information on Medicare utilization and cost for the dually eligible population even though these beneficiaries often were a significant part of the enrolled population.
The evaluators found sufficient data was available in Missouri to support a meaningful analysis of the program impacts on cost and utilization, and they completed such an analysis.45 The analysis distinguished among four subpopulations: Medicaid only enrollees in the primary care program; Medicaid only enrollees in the SMI program; dually eligible enrollees in the primary care program; and dually eligible enrollees in the SMI program. For Medicaid only enrollees in the primary care program, no statistically significant difference in spending was found indicating neither savings nor added expenses. Similarly, for dually eligible enrollees in the primary care program no statistically significant change in total spending was found, although the mix of spending shifted toward less Medicaid and more Medicare. For Medicaid only enrollees in the SMI program, spending increased about 15 percent relative to the comparison group, but savings were found for those who had been in the program for the longest duration suggesting continued enrollment of about two years might lead to savings. For dually eligible enrollees in the SMI program no statistically significant change in total spending was found, but (as with the Medicaid only group) savings were evident for those with the longest enrollment in the program.
Sufficient data were not available in the national evaluation to permit a quantitative analysis of health outcomes or the quality of care delivered. However, interviews with stakeholders yield this overall conclusion: “Importantly, providers in our evaluation states appreciated the benefits of health homes for their patients and were largely supportive of the model as a way to address the needs of Medicaid beneficiaries with physical and mental chronic conditions and complex socio- economic situations.” Additional conclusions were: “Most informants believe there have been improvements in the care enrolled members are receiving because of changes brought about by health homes and other delivery system reforms. In the areas of care coordination, integration of behavioral and physical health, and member engagement, our informants felt health homes were making continuous improvements. Transitional care, especially after hospitalizations, seems to be an area of ongoing concern for many states and providers, with some health home programs experiencing changes in the right direction and others still intensively working on improvements. Most health homes felt enrollees’ access to nonclinical services has improved during the course of the program, although few saw changes related to access to long-term services and supports, mostly due to relatively small proportion of their patients in need of them.”46
The More Recent Programs
Since 2013, 13 states and the District of Columbia launched HH programs; Kansas discontinued its program leaving 13 jurisdictions with newer HH programs.47 Five of these have two different HH models operating for different populations, making the total number of newer HH programs 18. Among these 18, four were launched in 2013, five in 2014, three in 2015, four in 2016, and two in 2017.
Nearly all the newer programs serve a limited population of individuals with SMI or other mental health conditions. Recent enrollment ranged from 350 in New Mexico to 6,700 in Connecticut. The major exception to this pattern is Washington State’s program launched in 2013 in 37 counties and extended statewide in 2017. It targets a broad population with multiple chronic conditions as well as those with mental health conditions. Its recent enrollment exceeded 90,000. The enrollment process is passive enrollment, with eligible clients assigned to a lead agency and considered enrolled unless they opt out.
The Washington program relies on a two-tiered set of organizations.48 The State assigns eligible clients to a Lead Agency, which is required to have a network of CBOs to provide the required services, and the Lead Agency must also contract with a qualified Care Coordination Organization (CCO), which provides the case management and coordination services. Statewide 82 CCOs operate serving varying jurisdictions. Each lead agency serves one or more of seven regions within the state. The Lead Agencies are five managed care plans, which serve their eligible members and have about 70,000 enrollees, and five other entities with about 20,000 enrollees including local public agencies serving the aged and nonprofit CBOs. The independent lead agencies serve the fee-for-service population (mostly dual eligibles). The CCOs must meet state standards which include mandatory training of the coordination employees through state established programs of in-person and webinar sessions. The state also prepares brochures and other marketing information for use by the Lead Agencies.
Payments are made to the Lead Agencies with different arrangements for the managed care plans and the others. The managed care plans receive monthly capitation rates for enrollees, and that rate is designed to include the cost of HH services for eligible members. That is, HH services are treated the same as other benefits with managed care plans at risk for cost controls and accountable for appropriate service delivery. The independent lead agencies are paid fees in three stages: (1) a one-time payment ($228) for initial contact, meeting and enrollment, and completion of a case management plan; (2) monthly payments ($155) for ongoing coordination and support including one face-to-face contact and other services; and (3) later monthly payments ($61) for coordination of services (including at least a monthly call and periodic face-to-face contacts) for patients who have achieved a degree of self-management. Lead Agencies may retain 10 percent of the fee and pay the rest to contracted CCOs.
Washington uses a performance metric of a monthly “engagement rate.” This rate is the share of the enrolled population who receive the appropriate service each month. The recent rate for the managed care plans is a disappointing 7 percent; the other lead agencies average about 20 percent. The poor performance is due in part to a shortage of CCO capacity, and the state is actively recruiting to expand the CCO network. The state has not made any estimates of savings attributable to the HH program.
General Observations
The wide variation in features of state HH programs and the absence of appropriate data relating to program performance and impact make it unwise to judge some programs more successful than others or to try to extract clear lessons for New York. However, it is useful to make three general observations that set a context for identifying options to improve New York’s program.
- Most state programs focus on a targeted population, most often involving those with SMI, and are of a scale much smaller and narrower than that in New York.
- Most states used enrollment processes and care arrangements that built upon existing relationships between PCMHs or care management agencies and eligible clients. New York’s top down model required contacts by agencies with which the potential client may have had no previous contact, and alternative outreach through the bottom up approach was needed to achieve substantial enrollment.
- States have undertaken limited evaluation activity. Hence, little is known about the cost effectiveness of different models of HHs for different subsets of the eligible population. The limited evidence suggests greatest effectiveness for those with SMI and with an extended period of continuous HH enrollment.
OPTIONS FOR DISCUSSION
New York’s HH program is uniquely ambitious. Its distinctive combination of features are its broad scope of priority enrollees and associated large scale and its reliance on broad networks of CBOs under a lead agency to serve as a HH for diverse populations with whom they may have had no prior relationship.
Efforts to develop and report performance measures and to evaluate program impacts were delayed and to date have yielded little guidance for reform. Accordingly, a priority initiative in the near future should be more attention and urgency to building and applying a database and analytic framework for assessing program impacts with attention to identifying the subpopulations which are likely to receive the greatest benefits from the program. This requires sophisticated research designs including comparison groups, adjustments for social determinants, and other factors that influence cost and outcomes. The evaluation underway by DOH and the National Center on Addiction and Substance Abuse is a promising tool for addressing these questions and renewed priority for generating and making available findings is warranted. Pending the fruits of such an effort, thought should be given to generating options for redesign of the program along its distinctive elements.
1. Better targeting of priority subpopulations
The currently enrolled population may differ in profile from the high acuity, high cost population initially identified for the program. The degree of mismatch, if any, cannot be known without data, which is not publicly available, comparing the two groups. However, the acuity data in Table 6 indicate more than half of recent enrollees are in the lower acuity category, and while a growing percentage, less than one in five has SMI and is enrolled in a HARP.
Two factors likely underlie the potential mismatch. First, the limited enrollment yield of the top down enrollment process and the reliance on other referrals to generate most of the current enrollment may have resulted in many individuals not in the high acuity, high cost category being enrolled. These individuals of course meet the federal standards for eligibility and cannot be refused enrollment. Second, the relatively wide State definition for the priority population and even wider federal definition of eligibility make eligible some individuals not assigned priority for whom a HH can provide benefits, but for whom the potential cost savings may be low or even negative. A reassessment of which subgroups should be assigned highest priority for enrollment, drawing on the evaluation and analysis recommended above, might better target the population to those with the greatest potential benefits and cost savings.
2. Greater reliance on specialized HH entities
Prior to the creation of specialized HHs for children, New York’s program relied on a set of specialized legacy providers with relatively limited enrollment and new networks serving a broad population to reach most of the expanded target population. This contrasts with the approach in many other states, which used as lead agencies providers with established relationships with distinct populations, and those target populations were notably smaller than New York’s. However, New York HHs had the advantage of working with established care management agencies that had ties to current patients. This enabled the HHs to use the bottom up enrollment process to expand enrollment.
The experience suggests enrollment efforts are most successful when outreach efforts are made by staff from agencies with which a client is familiar and at a time and location when the potential HH services seem most relevant. This can be accomplished by increased reliance on staff from existing specialized providers such as community health centers and mental health centers. The creation of additional HHs with agencies such as these as the lead entity might improve enrollment efforts without recreating the limitations of highly specialized care management arrangements.
3. Stronger ties between MCOs and HHs including full integration for serving some groups
A large percentage of current adult HH enrollees are members of a managed care plan. However some aspects of the MCO-HH relationship are problematic. Some MCO leaders feel they have little or no way to hold accountable the HHs to which they refer clients, and for some clients MCOs believe they could do better by contracting directly with a case management agency or even providing the care management with their own staff. Some HH leaders feel MCOs could be more effective partners if the information flow about emergency visits and hospital admissions was timelier, if their physician providers were more cooperative in relationships with HH staff, and if MCOs were more actively engaged with CBOs. The planned shift to value-based payments will enable some innovation in this relationship with opportunities for greater mutual accountability and cooperation. Pending such innovations efforts can be taken to facilitate and provide incentives for more productive interactions.
4. Alternative payment rates including options with reduced payment for adults reaching a duration of enrollment after which greater self-management should be practical
The rate schedule has already undergone multiple revisions, but opportunities for further improvement remain. Three issues can be addressed in future changes.
- Limited resources for bottom up outreach. While separate payments are made for outreach for top down referrals, this is not the case for other outreach efforts which are yielding the bulk of enrollment. HHs support these efforts with current resources including the top down outreach payments, but some additional payment for this work could be built into a future revised rate structure especially if top down outreach rates are further reduced.
- Remaining mismatches between acuity classification and actual cost of case management for some patients in the low acuity category. The shift to a three-tiered payment system and subsequent increase in low acuity rates are widely viewed as desirable refinements. However some low acuity patients require a large investment in case management time because of non-medical factors not reflected in acuity scores and shortcomings in the scoring and classification system. Some mechanism for recognizing this would be an improvement.
- Lack of time limits on under care payments may be devoting resources to clients who no longer need a high level of care management. Currently no time limit is placed on the period during which a client can remain a HH enrollee with the HH receiving the monthly payment for their level of acuity. However, case management and patient education often set as a goal better self- management by the patient. When this goal is achieved, resources may be wasted by continuing to support a more intense level of care management services. A tiered rate structure with lower rates for those having been successfully served over some extended period of time might be more cost-effective.
5. Centralized development of marketing materials to be used by multiple HHs, MCOs and other referral agencies and of training materials and programs for case management and coordination staff at multiple agencies
Two issues related to the relatively decentralized nature of the HH network are the lack of economies of scale in developing marketing materials and training programs. The former seem needed given the reported lack of understanding of HH services and benefits among potential clients (exacerbated by the sometimes misconstrued name “health homes”), and the latter could help overcome the perceived variability in the performance of HHs and case management agencies. The centralized mechanism could be direct initiatives by DOH or DOH support for activity by a coalition of stakeholder agencies who agree to share products. Some steps in this direction have already be taken with DOH development of training programs for staff of HHs serving children in administering assessment instruments and of educational material for HHs and other providers serving the HARP population.
6. New initiatives to encourage and speed interoperability of HH electronic record systems and MCO and provider electronic health records
Shared information is critical to effective care coordination. Unfortunately, under current arrangements the timely sharing of relevant information too often depends on interpersonal contacts by staff rather than shared access to a common patient information system. The federal and state governments have made large investments in the development of electronic medical records that could provide such shared information; New York has established a set of regional health information exchanges known as the Statewide Health Information Network for New York (SHIN-NY). The result to date has been disappointing in terms of creating systems that support shared use by multiple agencies. Instead, a fragmented system of sometimes incompatible systems has emerged; these systems may provide significant benefits to provider networks and insurance plans (and individual patients), but the fragmentation hampers the work of HHs. The creation by DOH of the Medicaid Analytic Performance Portal (MAPP) HH Tracking System is intended to provide common information about clients to HHs, but it has limited clinical information and is not linked to electronic medical records. Some HHs have worked with PPSs to advance integration of information among systems, and these efforts are still underway. A solution to this complex national problem is not simple or short run; nonetheless additional attention should be given by all stakeholders to ways in which better sharing of information can be facilitated.
This paper was prepared by Charles Brecher, Senior Advisor for Health Policy, and Patrick Orecki, Research Associate. They benefited from the cooperation of numerous Health Home and Managed Care Organization leaders who agreed to be interviewed and commented on a preliminary draft of the paper. The staff of the New York State Department of Health contributed by making available relevant data, agreeing to interviews, and commenting on a preliminary draft. The report was edited by Laura Colacurcio and formatted for publication by Kevin Medina.
Footnotes
- See: Charles Brecher and Mina Addo, What Ails Medicaid in New York: And Does the Medicaid Redesign Team Have a Cure? (Citizens Budget Commission, May 2016), https://cbcny.org/research/what-ails- medicaid-new-york-0.
- Patrick Orecki, Challenges of Enhancing Effective Engagement of Community Based Organizations in Performing Provider Systems, (Citizens Budget Commission, November 2017), https://cbcny.org/re- search/challenges-enhancing-effective-engagement-community-based-organizations-performing.
- Caitlin Thomas-Henkel, Taylor Hendricks, and Kelly Church, Opportunities to Improve Models of Care for People with Complex Needs: Literature Review (Center for Health Care Strategies, November 2015), www.chcs.org/media/HNHC_CHCS_LitReview_Final.pdf.
- Background information on ACA provisions from Kathy Moses and Brianna Ensslin, Seizing the Opportunity: Early Medicaid Health Home Lessons, Issue Brief (Center for Health Care Strategies, Inc., March 2014), and Medicaid Health Homes: Implementation Update, Fact Sheet (Center for Health Care Strategies, Inc., June 2017), www.chcs.org/resource/medicaid-health-homes-implementation-update/.
- Information on these programs is from Brenda Spillman, Barbara Ormond, Elizabeth Richardson, and Aaron Chalek, Medicaid Health Homes in New York: Review of Pre-Existing Initiatives and State Plan Amendments for the State’s First Health Homes Under Section 2703 of the Affordable Care Act, (Office of Disability, Aging and Long-Term Care Policy, August 2012), https://aspe.hhs.gov/system/files/ pdf/76656/HHOption-NY.pdf, and Elizabeth Patchias, Andrew Detty, and Michael Birnbaum, Imple- menting Medicaid Health Homes in New York: Early Experience (Medicaid Institute at United Hospital Fund, February 2013), https://uhfnyc.org/publications/880881.
- Information on the CIDP is from Charles Michalopoulos and others, Final Report on an Evaluation of Six Pilot Coordinated Care Projects for High-Needs Medicaid Recipients (MDRC, August 2014), www.mdrc. org/publication/final-report-evaluation-six-pilot-coordinated-care-projects-high-needs-medicaid.
- Information on PCMHs is from Gregory Burke, Advancing Patient-Centered Medical Homes in New York, Issue Brief (United Hospital Fund, December 2013), https://uhfnyc.org/publications/880951; and Gregory Burke, Recent Trends and Future Directions for the Medical Home Model in New York, Issue Brief (United Hospital Fund, August 2015), https://uhfnyc.org/assets/1424; and Gregory Burke, The Growth of Medical Homes in New York State, 2014 to 2016, Data Brief (United Hospital Fund, Septem- ber 2016), https://uhfnyc.org/publications/881155.
- New York State Department of Health, A Path toward Value Based Payment: Annual Update (June 2016), p. 18, www.health.ny.gov/health_care/medicaid/redesign/dsrip/2017/docs/2016-06_vbp_ roadmap_final.pdf.
- Centers for Medicare and Medicaid Services, “Medicare Shared Savings Program Fact Sheet,” (January 2018), www.cms.gov/Medicare/Medicare-Fee-for-Sevice-Payment/sharedsavingsprogram/ about.html.
- Information on New York ACOs from Gregory Burke and Suzanne Brundage, Accountable Care in New York State: Emerging Themes and Issues, Special Report (United Hospital Fund, April 2015), https:// nyshealthfoundation.org/resource/accountable-care-in-new-york-state-emerging-themes-and-issues/; and New York’s Medicare ACOs: Participants and Performance, Data Brief (United Hospital Fund, April 2015), https://nyshealthfoundation.org/wp-content/uploads/2017/11/new-york-medicare- acos-participants-and-performance.pdf; and United Hospital Fund, Health Watch, “New York Medi- care ACO Performance: Cost and Quality Results Raise Bigger Questions” (December 2017), https:// uhfnyc.org/publications/881264.
- Stacy Dale and others, “Two-Year Costs and Quality in the Comprehensive Primary Care Initiative,” New England Journal of Medicine (June 16, 2016), pp. 2345-2356, http://www.nejm.org/doi/ full/10.1056/NEJMsa1414953.
- Henry Ireys and others, Evaluating the CHIA – Behavioral Health/Substance Abuse Awards: Third Annual Report, Mathematica Policy Research (January 23, 2017), https://downloads.cms.gov/files/cmmi/hcia-bhsa-thirdannualrpt.pdf.
- Henry Ireys and others, Evaluating the CHIA – Behavioral Health/Substance Abuse Awards: Addendum to the Third Annual Report, Mathematica Policy Research (July 14, 2017), www.mathematicampr. com/our-publications-and-findings/publications/evaluating-the-hcia-behavioral-health-substance- abuse-awards-addendum-to-the-third-annual-report.
- New York’s Medicare ACOs: Participants and Performance, Data Brief (United Hospital Fund, April 2015), p. 7, https://nyshealthfoundation.org/wp-content/uploads/2017/11/new-york-medicare-acos-participants-and-performance.pdf.
- Data in this paragraph from US Department of Health and Human Services, Exploring Medicaid Health Homes: New York: Transforming Care Delivery via Health Homes (March 12, 2012), pp. 22 and 24, www. medicaid.gov/state-resource-center/medicaid-state-technical-assistance/health-homes-technical- assistance/downloads/health-homes-slide-binder-march-2012-508.pdf.
 The New York State Office for People with Developmental Disabilities will launch a care coordination effort for individuals with developmental disabilities beginning in July 2018. See: New York State Office for People with Developmental Disabilities, “Frequently Asked Questions (FAQ) About Care Coordination Organizations/Health Homes (CCO/HH)” (accessed March 19, 2018), https://opwdd.ny.gov/opwdd_services_supports/care_coordination_organizations/faq.
The New York State Office for People with Developmental Disabilities will launch a care coordination effort for individuals with developmental disabilities beginning in July 2018. See: New York State Office for People with Developmental Disabilities, “Frequently Asked Questions (FAQ) About Care Coordination Organizations/Health Homes (CCO/HH)” (accessed March 19, 2018), https://opwdd.ny.gov/opwdd_services_supports/care_coordination_organizations/faq. U.S. Department of Health and Human Services, Exploring Medicaid Health Homes: New York: Transforming Care Delivery via Health Homes (March 12, 2012), page 28, www.medicaid.gov/state-re- source-center/medicaid-state-technical-assistance/health-homes-technical-assistance/downloads/ health-homes-slide-binder-march-2012-508.pdf.
U.S. Department of Health and Human Services, Exploring Medicaid Health Homes: New York: Transforming Care Delivery via Health Homes (March 12, 2012), page 28, www.medicaid.gov/state-re- source-center/medicaid-state-technical-assistance/health-homes-technical-assistance/downloads/ health-homes-slide-binder-march-2012-508.pdf.- U.S. Department of Health and Human Services, Exploring Medicaid Health Homes: New York: Transforming Care Delivery via Health Homes (March 12, 2012), p. 30, www.medicaid.gov/state-resource-center/medicaid-state-technical-assistance/health-homes-technical-assistance/downloads/health- homes-slide-binder-march-2012-508.pdf.
- Unpublished data provided by New York State Department of Health, email to CBC staff (April 19, 2018).
- New York State Department of Health, State Plan Amendment #11-56 (January 27, 2012), pp. 15- 20, www.health.ny.gov/regulations/state_plans/status/non-inst/approved/docs/app_2012-02-03_ spa_11-56.pdf.
- The downstate region includes New York City, Dutchess, Nassau, Orange, Putnam, Rockland, Suffolk and Westchester counties.
- New York State Department of Health, “Introducing Health Homes” Medicaid Update, Special Edition, Volume 28, Number 4 (April 2012), p. 10, www.health.ny.gov/health_care/medicaid/program/ update/2012/2012-04_pharmsped_edition.htm.
- Brenda Spellman, Barbara A. Ormond, Elizabeth Richardson, and Aaron Chalek, Medicaid Health Homes In New York: Review Of Pre-Existing State Initiatives And State Plan Amendments For The State’s First Section 2703 Medicaid Health Homes (Urban Institute, August 2012), p. 9, https://aspe.hhs.gov/ system/files/pdf/76656/HHOption-NY.pdf.
- New York State Department of Health, Health Homes Provider Manual–Billing Policy and Guidance (May 20, 2013), p. 28, www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/ docs/hh_prov_manual.pdf.
- New York State Department of Health, State Plan Amendment #14-16 (March 10, 2015), www.health. ny.gov/regulations/state_plans/status/non-inst/approved/docs/app_2015-03-10_spa_14-16.pdf; and New York State Department of Health, New York Partnership Plan Waiver number 11-W-00114/2 (April 2014), p. 65, www.health.ny.gov/health_care/managed_care/appextension/docs/2014-07- 07_waiver_authority_stcs.pdf.
- HARPs are managed care plans which integrate physical health, mental health, and substance abuse treatment for high needs beneficiaries. See: New York State Department of Health, “Health and Recovery Plan (HARP)/ Behavioral Health” (October 2017), www.health.ny.gov/health_care/medicaid/ program/medicaid_health_homes/harp_bh/index.htm.
- New York State Department of Health, “Health Home Plus (HH+) and Health Home Plus Expansion” (September 2017), www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/ special_populations/hh_plus.htm.
- New York State Department of Health, State Plan Amendment #13-18 (March 26, 2013), p. 25, www. health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/spa13-18.pdf.
- New York State Department of Health, State Plan Amendment #13-63 (September 19, 2014), www. health.ny.gov/regulations/state_plans/status/non-inst/approved/docs/app_2014-09-19_spa_13- 63.pdf, New York State Department of Health, State Plan Amendment, #15-20 (April 14, 2016), www. health.ny.gov/regulations/state_plans/status/non-inst/approved/docs/app_2016-03-28_spa_15- 20.pdf, and New York State Department of Health, State Plan Amendment # 16-34, (December 22, 2016), www.health.ny.gov/regulations/state_plans/status/non-inst/approved/docs/app_2016-12- 22_spa_16-34.pdf.
- New York State Department of Health, Modifications to Health Home Outreach: Guidance and Preliminary Timeline, (September 25, 2017), www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/outreach_reprogramming_guidance_10_1_17.pdf.
- New York State Department of Health, “Dashboard B9,” (accessed February 10, 2018), https://dsrip- dashboards.health.ny.gov/.
- New York State Department of Health, Temporary Health Home Billing Procedures effective December 1, 2016, (September 2016), www.health.ny.gov/health_care/medicaid/program/medicaid_health_ homes/docs/temp_bill_procedures.pdf.
- New York State Department of Health, “DHDTC DAL 17-04 - Hospital Requirements for Making Referrals to Health Home” (February 15, 2017), www.health.ny.gov/professionals/hospital_adminis- trator/letters/2017/2017-02-15_dal_17-04_req_making_referrals_to_hh.htm.
- New York State Department of Health, Health Homes Serving Children CANS-NY and Billing Guidance (June 29, 2016), p. 4, www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/ docs/june_29_2016_billing_guidance_final.pdf
- New York State Department of Health Office of Health Insurance Programs, NYS Health Home Performance Management and Quality Measures (May 10, 2017), www.health.ny.gov/health_care/medicaid/ program/medicaid_health_homes/assessment_quality_measures/docs/performance_mana_qual- ity_measures.pdf.
- New York State Department of Health Office of Health Insurance Programs, Health Home Performance (January 24, 2018), www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/ webinars/docs/2018_01_24_hh_performance_webinar.pdf.
- New York Health Home Coalition, Letter to Peggy Elmer (February 26, 2018)
- Center for Health Care Strategies, Medicaid Health Homes: Implementation Update, Fact Sheet (June 2017) www.chcs.org/resource/medicaid-health-homes-implementation-update/.
- Brenda Spillman and others, Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Progress and Lessons from the First States Implementing Health Home Programs, Annual Report- Year Four (Urban Institute, April 2016), https://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-progress-and-lessons-first-states- implementing-health-home-programs-annual-report-year-four.
- Dan Shae, Phuong Nguyen-Hoang, Suzanne Bentler, Peter Damiano, and Elizabeth Momany, “Medicaid Health Home Reducing Cost and Reliance on Emergency Department: Evidence from Iowa,” Medical Care, vol. 54, no. 8, (August 2016) pp. 752-757.
- Brenda Spillman and others, Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Progress and Lessons from the First States Implementing Health Home Programs, Annual Report- Year Four, (Urban Institute, April 2016), p. 4, https://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-progress-and-lessons-first- states-implementing-health-home-programs-annual-report-year-four.
- Brenda Spillman and Eva Allen, Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Evaluation of Outcomes of Selected Health home Programs, Final Annual Report: Year Five, (Urban Institute, May 11, 2017), p. 41, https://aspe.hhs.gov/pdf-report/evaluation-medicaid-health-home- option-beneficiaries-chronic-conditions-evaluation-outcomes-selected-health-home-programs-annual-report-year-five.
- Brenda Spillman and Eva Allen, Medicaid Health Home Option for Beneficiaries with Chronic Condi- tions: Evaluation of Outcomes of Selected Health home Programs, Final Annual Report: Year Five, (Urban Institute, May 11, 2017), p. A-8, https://aspe.hhs.gov/pdf-report/evaluation-medicaid-health-home- option-beneficiaries-chronic-conditions-evaluation-outcomes-selected-health-home-programs-annual-report-year-five.
- Brenda Spillman and others, Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Progress and Lessons from the First States Implementing Health Home Programs, Annual Report- Year Four, Urban Institute, April 2016, p. 48, https://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-progress-and-lessons-first- states-implementing-health-home-programs-annual-report-year-four.
- Brenda Spillman and Eva Allen, Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Evaluation of Outcomes of Selected Health home Programs, Final Annual Report: Year Five, (Urban Institute, May 11, 2017), pp. 14-26, https://aspe.hhs.gov/pdf-report/evaluation-medicaid-health-home- option-beneficiaries-chronic-conditions-evaluation-outcomes-selected-health-home-programs-annual-report-year-five.
- Brenda Spillman and others, Evaluation of the Medicaid Health Home Option for Beneficiaries with Chronic Conditions: Progress and Lessons from the First States Implementing Health Home Programs, Annual Report- Year Four (Urban Institute, April 2016), p. viii, https://aspe.hhs.gov/basic-report/evaluation-medicaid-health-home-option-beneficiaries-chronic-conditions-progress-and-lessons-first- states-implementing-health-home-programs-annual-report-year-four.
- Information in this section from Health Home Information Resource Center, Center for Medicare and Medicaid Services, Medicaid Health Homes: An Overview, (May 2017) and Medicaid Health Homes: SPA Overview (May 2017), www.medicaid.gov/state-resource-center/medicaid-state-technical-assis- tance/health-home-information-resource-center/index.html.
- Information on Washington’s program from Washington State Health Care Authority, “Washington State Health Home Program Coming to King and Snohomish Counties” (August 2016), (accessed February 2, 2018), www.youtube.com/watch?v=HnfY8a_7Mcc; and telephone interview with Karen Fitzharris, Washington State Department of Health and Social Services (February 7, 2018).